
Case Report | DOI: https://doi.org/10.31579/2578-8868/108
1 MD Candidate Class of 2020, Faculty of Medicine, University of Toronto, 1 King’s College Circle, Medical Sciences Building, Toronto, Ontario Canada, M5S 1A8.
2 MD, Saba University School of Medicine, Church Street, The Bottom, Saba, Dutch Caribbean, Netherlands, P.O. Box 1000.
3 Department of Medicine, Division of Neurology, Service of Neuro-Oncology, Princess Margaret Cancer Centre, 610 University Avenue, Pencer Brain Tumor Centre, 18th Floor, University Health Network, University of Toronto, Ontario, Canada, M5G 2M9.
4 Department of Medicine, Division of Neurology, Service of Neuro-Oncology, Princess Margaret Cancer Centre, 610 University Avenue, Pencer Brain Tumor Centre, 18th Floor, University Health Network, University of Toronto, Ontario, Canada, M5G 2M9.
*Corresponding Author: atherine Maurice, Neuro-Oncologist, University of Toronto Princess Margaret Cancer Centre Toronto, ON, Canada.
Citation: Austin M. Pereira., Amanda K. Pereira., Warren P. Mason., Maurice C. (2019) Ataxia Following Allogenic Stem Cell Transplantation: No Stone Unturned. J. Neuroscience and Neurological Surgery. 5(2); DOI:10.31579/2578-8868/108
Copyright: © 2019 Catherine Maurice, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any Medium, provided the original author and source are credited.
Received: 02 December 2019 | Accepted: 13 December 2019 | Published: 17 December 2019
Keywords: ataxia; graft versus host disease; allogenic transplantation; anti-tr; anti-gad; opportunistic infections; neuroimmunology; pan-cerebellar syndrome; acute myeloid leukemia; clinical investigation
A thirty-one year-old Sri Lankan man presented with a two-month history of progressive pan-cerebellar syndrome, following allogeneic stem cell transplantation. This curative-intent therapy was performed in the context of an underlying acute myeloid leukemia. During the post-transplant period, patients are extremely vulnerable, especially due to the immunologic fluctuations. Reaching equilibrium is crucial, preventing complications of both extremes of the immunologic response, such as opportunistic infections or graft versus host disease. Numerous aetiologies were considered in the differential diagnosis of this pan-cerebellar syndrome. Most of those conditions mandate a prompt management, because of their reversible or lethal nature. Our thorough investigation process was a race against time. Excluding “Red Flags” remains the priority. Mindfulness and time will eventually lead to the proper diagnosis. We discuss our structured investigation process emphasizing on the key element: a “Systematic Approach”.
Running Title: Ataxia post stem cell transplant
A thirty-one year-old Sri Lankan man presented at the neuro-oncology clinic of Princess Margaret Cancer Centre for the investigation and management of a pan-cerebellar syndrome, progressively evolving for two months, following allogeneic stem cell transplantation. This curative-intent procedure was performed two years after a diagnosis of acute myeloid leukemia (AML). His initial therapy consisted of standard chemotherapy including: cyclophosphamide, cytarabine, doxorubicin and methotrexate. His family history was unremarkable for consanguinity, hereditary or metabolic conditions. Unfortunately, during the post-transplant period, this gentleman developed a multi-systemic graft versus host reaction (GVHD) involving his eyes, liver, skin and lungs. Reaching an immunologic equilibrium during this vulnerable period is challenging. The GVHD treatment induced an iatrogenic state of profound immunosuppression, leading to the development of multiple opportunistic infections. The central nervous system (CNS) resides in a sanctuary, protected by the blood brain barrier (BBB); it remained unaffected throughout this period of fragility.
We were facing an extensive differential diagnosis [1] [Table 1], considering the presence of an underlying hematologic malignancy, the post-transplantation context associated with immunologic fluctuations, the coexistence of recent complications, namely multi-systemic GVHD and opportunistic infections. We also thought about any aetiology potentially responsible for the development of a pan-cerebellar syndrome in a young adult, manifesting as a sudden outburst in a state of extreme fragility.
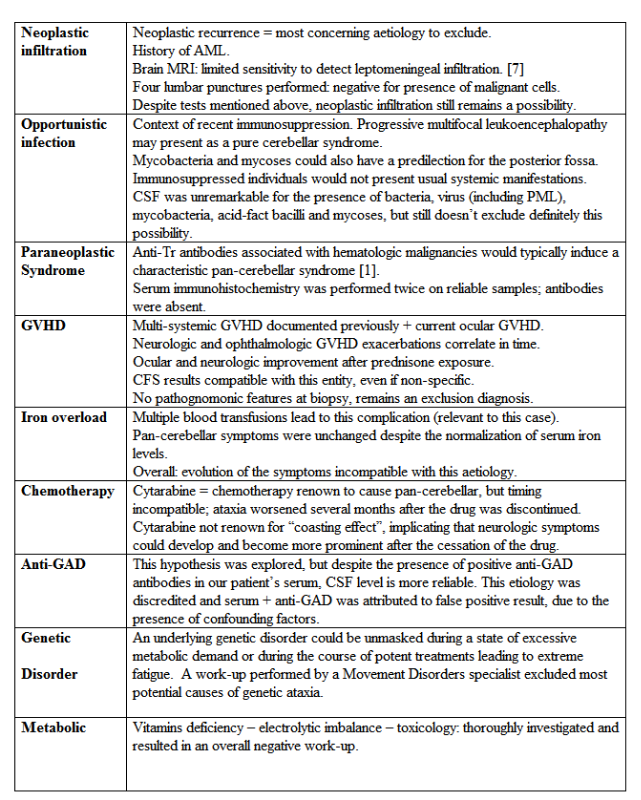
Table 1. Differential Diagnosis of Pan-Cerebellar Syndrome Investigated: Context of AML - Post Stem Cell Transplantation
After a thorough investigation as described in Table 1, GVHD became our main working diagnosis. The pan-cerebellar syndrome was characterized by the following findings at the clinical examination: symmetrical diffuse axial and appendicular ataxia impacting gait, symmetrical adiadochokinesia, bilateral dysmetria and dysrythmia involving upper and lower limbs, cerebellar dysarthria and downbeat nystagmus. Cranial nerves were otherwise within a normal range. The motor and sensory modalities were preserved.
Reflexes were unaffected, except the presence of pendular reflexes at bilateral patellar sites. A subtle cerebellar intention tremor involved symmetrically bilateral upper limbs. There were superimposed ocular manifestations, such as keratosis, erythema and pruritus. After a specialized ophthalmologic investigation, those features were attributed to concomitant ocular GVHD. Moreover, a skew deviation was attributed to a contiguous brainstem involvement. Isolating the precise nature of each of ocular phenomenon was key in this investigation process. The parallel course of the ocular GVHD and the cerebellar/brainstem symptoms, flaring-up and improving at the exact same time, was the most important element suggesting the diagnosis of CNS GVHD, involving the posterior fossa. In addition, we noticed that administration of oral prednisone lead to an improvement of both neurologic and ocular manifestations. We would expect the opposite reaction in presence of opportunistic infection.
Our gentleman was prescribed azathioprine, 200 mg PO when GVHD became our main working hypothesis, and the presence of opportunistic infections was excluded. Azathioprine was selected aiming a long-term treatment, and a well-tolerated side-effect profile. However, we acknowledge that this drug could take up to nine months to show the first signs of improvement. Seven months later, the ataxia was still unchanged. The challenge is to be absolutely certain to have excluded without a doubt the presence of malignancy or opportunistic infections involving the posterior fossa. Those two reversible aetiologies remain untreated during the azathioprine trial, and warrant a prompt management, to avoid preventable lethality. The role of a brain biopsy was controversial and was discussed extensively during multidisciplinary tumor boards. It represents the only modality to exclude without a doubt an infectious or neoplastic process undiagnosed by lumbar puncture. In this specific context, a brain biopsy is associated with high morbidity and could generate fatal complications. [2,3] The decision mainly relied on the patient’s clinical status, permitting a biopsy in his current state, which could have deteriorated afterwards. We weighted thoroughly the risks and benefits of such a procedure, and finally ruled in favour of the biopsy.
The pathology analysis was finally compatible with a previous inflammatory process, currently in resolution. The presence of residual polyclonal lymphocytic infiltrates within the perivascular space suggested the presence of resolving inflammation. This description is compatible with GVHD, but it is not pathognomonic. The absence of infectious agents or neoplastic features was extremely reassuring and we proceeded by resuming azathioprine. We noted a clinical improvement after nine months of azathioprine treatment, which consolidated our diagnosis of CNS GVHD [4-6].
Numerous neurologic complications could arise from hematopoietic stem cell transplantation. The challenging aspect of this case is the definite exclusion of treatable conditions [3]. We presented this case to highlight a reality: every physician will face “unknown territories”, and scenarios we never specifically learn to manage. We can’t be wrong if we rely on our judgement, adopt a systematic approach, and remember that we are never alone, consultants are there for a reason. If the patient understands the reflection process, the logic standing behind every action, and ideally takes part to the discussion, the relationship patient-physician will be optimal and both parties will be reassured to crossing the “unknown territories” together.

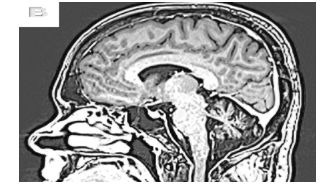
Brain MRI performed 6 months following pan-cerebellar syndrome onset:
Disclosures:
vNo Sponsorship was received for the redaction of this manuscript.;
vThe authors did not receive any financial compensation.
vThe authors did not receive any research support.
vThe authors do not have any stocks, stock options or royalties in the medical industry.
vThe authors are not involved in legal proceedings related to the content of this manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
